
Issue 247 – 11 June 2026

|
Welcome to Practice Connect, a fortnightly update for practice managers, principals, nurses and administration staff on relevant issues, upcoming events and education. |
Quality improvement and data
Data cleansing and archiving: The essential first step for accurate, data led quality improvement

Data-led quality improvement (QI) is central to how general practices plan, measure and improve care. Whether undertaking preventative health initiatives, reviewing Chronic Disease Management, or responding to new program requirements, the quality of the outcome is only as strong as the quality of the underlying data.
One of the most effective, yet often overlooked, starting points is data cleansing and archiving.
Why start with data cleansing?
Over time, practice databases naturally accumulate records for patients who have moved, transferred to another practice, or are no longer actively attending. If these records remain active, they can unintentionally impact the accuracy of practice data, reporting and patient communications.
Data cleansing and archiving help practices to:
- Improve the accuracy of population health reporting
- Streamline QI audits and data led initiatives
- Ensure recalls and reminders are targeted appropriately
- Reduce unnecessary patient contact
- Increase staff confidence in data outputs
By focusing on patients who are actively engaging with the practice, QI activities become more meaningful and reflective of real world care delivery.
The RACGP Standards for general practices (5th edition) C7.1 reference the importance of understanding a practice’s active patient population to support clinical governance, continuous improvement and patient centred care. Maintaining a clear distinction between active and inactive patients supports safer systems, clearer performance insights and more effective planning.
Common practice hesitation
A common misconception is that archiving inactive patients may impact practice incentive measures, such as the Standardised Whole Patient Equivalent (SWPE). However, SWPE is based on Medicare Benefits Schedule (MBS)‑billed services processed by Medicare, not on whether a patient record is marked as active or inactive within practice software.
Embedding data cleansing into everyday QI
Rather than a one-off exercise, data cleansing and archiving work best when they are embedded into regular QI cycles and supported by clear practice processes.
For practices starting or refreshing their QI journey, archiving inactive patients is a practical and powerful first step, creating a strong foundation for all future data-led initiatives.
The WA Primary Health Alliance (WAPHA) team of dedicated Quality Improvement Coaches are happy to assist with tailored QI support and development of activities for your practice. If you would like a QI Coach to provide your team support contact us via our email qi@wapha.org.au
Access the PDSA: Archiving inactive patients (generic software)
Quality improvement (QI) webinars:
Catch up on previous webinar sessions by visiting the Quality Improvement YouTube series.
![]()
View our QI Bites videos – Primary Sense in Practice:
- Video 1: Accreditation Report
- Video 2: Health Assessments Report
- Video 3: PIP QI 10 Measures Report
- Video 4: CVD Patients for Screening, Recall and Treatments Report
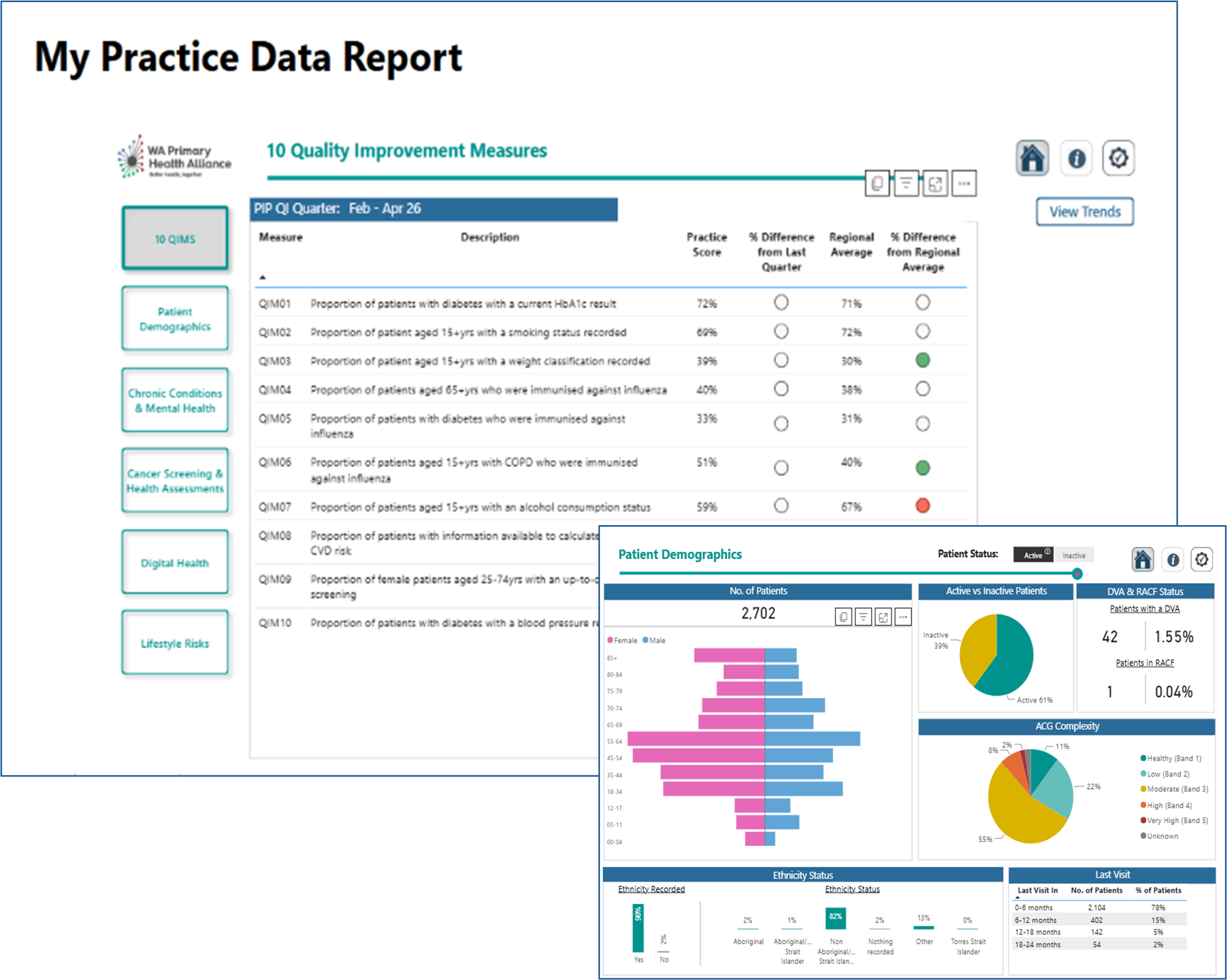
My Practice Data report – Are you getting the most out of your data?
The Primary Care Reporting Portal (PCRP) is available to general practices who have Primary Sense and in today’s evolving environment, access to clear and timely data has never been more important.
PCRP is designed to give practices a simple way to view and understand their practice data and provides some comparison to regional averages.
The PCRP gives you visibility over key Quality Improvement Measures (QIMs), evolving trends, areas for improvement and opportunities for preventative health activities including immunisation and cancer screening.
By understanding your data, you can identify opportunities to optimise outcomes and business sustainability.
WA sits below the national average in relation to immunisation. Using Primary Sense and PCRP together we can identify areas for improvement within general practice to make a significant impact.
Access your My Practice Data Report today and start identifying priority areas and insights to guide positive patient outcomes.
If you need support, your Primary Care Navigator can assist with accessing your report, understanding your data, identifying improvement opportunities and linking insights to practical actions through referral to your QI coach.
Contact your Primary Care Navigator or alternatively email Practice Assist or phone 08 6278 7900.
Practice news
Primary Sense – Best Practice Halo Connect Integration action required by 30 June 2026
General practices that use Best Practice (BP) Premier practice management software will need to take immediate action to ensure continued connectivity with the Primary Sense data extraction and clinical decision support tool.
Halo Connect is the supported method for enabling secure, real-time access between BP Premier and Primary Sense.
Primary Sense extractions will cease if Halo Connect integration is not completed by 30 June 2026. This will impact on PIP QI data submissions and in-practice use of Primary Sense for reports, prompts and alerts.
Communications have been sent to all WA practices impacted by this change along with detailed instructions to successfully complete the connection. Alternatively see the Primary Sense Best Practice Halo Connect Practice Guide for step-by-step instructions.
For further support please contact primarysense@wapha.org.au, your Primary Care Navigator or call Practice Assist on 08 6278 7900.
New Support at Home Program resources to help navigate referrals
The Australian Government Department of Health, Disability and Ageing has released new resources to support conversations with older patients about the short-term Support at Home Program* pathways available to help older people remain at home as they age:
These materials are designed to provide clear, practical guidance on eligibility, referral pathways and where to find further information.
The End-of-Life Pathway GP flyer has been developed in response to sector feedback calling for concise guidance on patient eligibility and referral processes.
The Support at Home flyer is also available to help general practice teams understand how patients can be referred to access Support at Home services, with links to additional information for clinical and primary care settings.
The DHDA has also released a new Support at Home short-term pathways video, now available via the My Aged Care website. The video explains how the program’s three short-term pathways work alongside, or instead of, ongoing services and may be useful when discussing options with older patients and carers. It is also available in translated formats, including Auslan.
More information for health professionals is available on the DHDA website.
*The Support at Home Program replaced the Home Care Packages Program and Short-Term Restorative Care Programme in November 2025 and includes both ongoing care and three short-term pathways.
Driving better care through the MedicineInsight Program

MedicineInsight offers a unique opportunity for general practitioners and practices to embed data-driven insights into their daily practice.
Formerly operating under NPS MedicineWise, the MedicineInsight program is a national program now delivered by the Australian Commission on Safety and Quality in Health Care. The program supports quality improvement in primary care by securely using data from Australian general practices to promote best practice, enable post-market observation of medicines and support ongoing primary care research that informs policy, guidelines and safer patient care nationwide.
Why register your practice?
Participation in the MedicineInsight program delivers meaningful benefits for both practices and individual GPs:
- Free to join– no cost to the practice or clinicians
- Individualised Practice Reports and customised GP-level Reports
- Access to the MedicineInsight dashboard, a secure online platform with:
- Monthly updated data
- Comparison against the aggregate data of all participating practices
- Reports that support quality improvement activities and contribute to RACGP and ACRRM accredited Continuing Professional Development (CPD) hours.
- Strong data governance and privacy protections:
- All data is fully de-identified
- Data is never sold or used for commercial gain
The MedicineInsight program is the only national, longitudinal data collection with RACGP Ethics approval.
Join today:
Join the growing number of practices and GPs already benefiting from MedicineInsight and helping to strengthen the evidence base for Australian primary care.
Click here to register and get started today.
For more information contact MedicineInsight@safetyandquality.gov.au
Electronic prescribing and active script lists – Are lost prescriptions impacting your practice?

Electronic prescribing (EP) provides a secure, fast and efficient way for patients to receive medication prescriptions. EPs can be issued during an in-person or telehealth consultation and sent directly to the patient’s mobile phone or email. EPs are available nationally either as a ‘token’ (via SMS or email) or through an Active Script List (ASL).
An Active Script List (ASL) is a token management solution. It is a consolidated list of all the patient’s active electronic prescriptions (e-scripts) including repeats. After the patient registers for an ASL at a pharmacy, they can authorise any pharmacy to access and dispense their e-scripts from their ASL without needing to display the QR token.
ASL makes medication management easier for patients:
- Taking multiple medications regularly
- That lose or struggle to keep track of their paper or electronic prescriptions
- Without smartphones
- With chronic conditions or who rely on carers or support people to assist with medication collection
Further information:
- EP overview for prescribers
- Software conformance register
- Training on EP and ASL in your practice
- Video: Managing multiple EPs using the ASL
For more information or support on setting up and using e-scripts in your practice, contact the Practice Assist on 08 6278 7900 or via email practiceassist@wapha.org.au
Alert for WA clinicians – Ebola disease update in Central and Eastern Africa
The World Health Organization has determined that the ongoing outbreak of Ebola disease caused by Bundibugyo virus (BVD) in the Democratic Republic of the Congo (DRC) and Uganda constitutes a Public Health Emergency of International Concern under the International Health Regulations (2005).
Although this outbreak currently presents a low risk to Australia, health care workers are advised to remain vigilant for the signs and symptoms of Ebola.
Key points from the WA Health Alert for Clinicians 26 May 2026:
- At triage or reception, identify patients with fever, with or without additional symptoms of Ebola disease, and travel history to affected areas of DRC or Uganda in the 21 days prior to symptom onset
- Immediately isolate patients meeting these criteria in a negative pressure isolation room or single room with the door closed. Apply standard, contact, droplet and airborne precautions; refer to the viral haemorrhagic fever (VHF) infection prevention and control (IPC) interim guideline for specific PPE advice
- Urgently discuss with the local public health physician or call 1800 434 122 if after-hours
- Asymptomatic health or aid workers returning from affected areas should already be known to Public Health for symptom monitoring. Notify Public Health Unit of other returned travellers with high-risk exposures
Further resources from the Australian Centre for Disease Control:
- Infection prevention and control principles and recommendations for Ebola virus disease
- CDNA National Guidelines for Public Health Units
Ebola information for frontline health professionals.
Read the full alert here.
MyMedicare and Medicare updates
Assignment of Benefit updates for Medicare bulk billing

The Department of Health, Disability and Ageing (DHDA) is progressing work to develop digital solutions aimed at improving Medicare payment processes. These enhancements are intended to increase transparency for patients while strengthening the integrity of the Medicare system.
A key component of this reform is the introduction of updated Assignment of Benefit (AoB) processes for all Medicare bulk billed services, which will commence on 1 July 2026.
The DHDA aim is to create solutions that will streamline Medicare billing for bulk billed services and simplified billing services.
Changes occurring from 1 July 2026
- Verbal AoB will no longer be available
- Patients can assign benefits before or after a service, provided consent is obtained prior to submitting an MBS claim
- The requirement for an ‘approved form’ and practitioner signature will be removed, however agreements must still meet legislative data requirements
- A patient (or responsible person) must provide an identifiable and auditable electronic or physical signature, compliant with the Electronic Transactions Act 1999
- Practices are required to retain AoB agreements for two years and provide a copy to the patient upon request
Aged Care
These Assignment of Benefit changes will also apply in aged care and may affect how care is delivered to residents. The DHDA has outlined these impacts in its FAQ document.
An AoB will still be required for bulk billed services provided in aged care homes. If a resident does not have capacity to make financial or health decisions, an authorised representative may consent on their behalf. Under the Health Insurance Act 1973, this is generally a carer, partner, parent or a person holding Power of Attorney.
The Department is also finalising arrangements for an enduring AoB for eligible patients, including those registered with MyMedicare or receiving care through an Aboriginal Community Controlled Health Organisation (ACCHS) or Aboriginal Medical Service (AMS). This would allow a single agreement, signed by the patient or their assignor, to cover future services provided by a nominated practice.
Enduring AoB is expected to commence in 2027 and will require providers to notify patients after each service.
Resources
- Assignment of Medicare Benefits for Bulk Billing
- Improving the assignment of benefit process
- Assignment of benefit for bulk bill claims – Health professionals
- Assignment of Medicare Benefits for Bulk Billing – Frequently Asked Questions
- Assignment of Medicare Benefits for Simplified Billing – Frequently Asked Questions
- Modernising the Assignment of Benefit Process
Education and Learning
- Medicare Assignment of Benefit changes for bulk billing: a guide for practices (Tyro Health)
- Preparing your practice for the new Assignment of Benefit changes (Cubiko)
- Assignment of Benefit and our Oxford Release (Best Practice)
- Assignment of Benefit and Sender ID Resources (Best Practice)
Next steps
- Consider how pre- and post-assignment can be incorporated into your practice workflow
- Contact your software provider to discuss how this integration will work
If you would like to provide feedback or ask further questions, please contact the Australian Government Department of Health, Disability and Ageing on AssignmentofBenefit@health.gov.au
For further support please contact Practice Assist or your Primary Care Navigator on 08 6278 7900 or via email practiceassist@wapha.org.au
1800MEDICARE resources now available

1800MEDICARE is a free, 24/7 government-funded service for non-emergency health advice that can be accessed via phone (1800 633 422), website and smartphone app (formerly the my health app).
The service is available to everyone in Australia, no Medicare card is required. Calls are answered by a registered nurse with clinical experience, who will listen to concerns and assess symptoms using clinical decision support tools and provide evidence based advice.
The service can help when someone:
- Is unsure if they need medical help
- Needs advice for a non-emergency health concern
- Wants help finding services in their area
For further information, refer to the 1800MEDICARE resources:
MyMedicare program updates and resources
The MyMedicare Registration Form and Program Guidelines have been updated and are available on the Department of Health, Disability and Ageing (DHDA) website from 2 June 2026. Services Australia systems have also been updated to align with the revised form.
The updates clarify guidance for practices on consent for incapacitated persons and exemptions for extenuating or unforeseen circumstances. They mainly apply to:
- Section 7.4 – Incapacitated Persons (consent) provisions
- Section 6.4.2 – Extenuating or unforeseen circumstances exemptions
Updated brochures and practice posters are now available.
Printed copies can be ordered from National Mailing and Marketing by emailing health@nationalmailing.com.au or calling 02 6269 1080 and quoting Order ID: A01006.
Access the full range of MyMedicare resources here.
For additional information and support on MyMedicare contact Practice Assist or your Primary Care Navigator on 08 6278 7900 or via email practiceassist@wapha.org.au
MyMedicare Minute from the Department of Health, Disability and Ageing
|
MyMedicare Minute – Seven One key message. One minute to read. |
Registering patients who may lack capacity |
| MyMedicare registration is voluntary and requires informed consent.
In some circumstances, a patient may be unable to provide consent due to limited or impaired decision-making capacity. In these cases, a registration may be completed by the patient’s authorised representative. What to do first:
What practices need to know:
Resources
|
Immunisation updates
New mpox cases reported in WA
WA Health is reminding Western Australians to stay alert to mpox symptoms following notification of 7 new cases in a week. The new cases bring the total number reported in Western Australia so far in 2026 to 22 which is rapidly approaching the total number of cases reported for the whole of 2025 (27) and 2024 (23).
Most cases have been locally acquired, with investigations and contact tracing underway to prevent further spread. In Australia, mpox has primarily affected sexually active gay, bisexual and other men who have sex with men. However, recent cases have also included heterosexual men and, for the first time in WA, cisgender women.
A 2-dose schedule of mpox vaccine is recommended for people at higher risk of exposure. The vaccine is also recommended to be given within 14 days of exposure to help prevent infection or reduce the severity of illness.
Read the WA Health alert here.
Updates to disease chapters in the Australian Immunisation Handbook
The Respiratory Syncytial Virus (RSV) chapter of the Australian Immunisation Handbook (AIH) was updated on 12 May 2026 to include:
- Updated information on the expanded national RSV program, including Arexvy for adults aged ≥75 years and Aboriginal and Torres Strait Islander adults aged ≥60 years
- Clearer advice on the timing of RSV-specific monoclonal antibodies for infants and co-administration for older adults
- Editorial revisions to simplify guidance on RSV vaccination during pregnancy
- Evidence on the effectiveness and efficacy of the Arexvy vaccine in older adults
- Guidance on RSV immunisation product administration errors
Australian Immunisation Handbook app
The Australian Immunisation Handbook app is available on mobile devices and tablets, making it easier to use in clinical settings. It works offline and includes bookmarks, search, filtering and sharing functions. When connected, the app updates automatically so content, tables and resources remain current and accessible offline.
IOS – Immunisation Handbook App – App Store
Android – Search for the Immunisation Handbook app on the Google Play Store
Changes to the adult pneumococcal vaccination program from 1 July 2026
The Australian Government Department of Health, Disability and Ageing has announced updates to the adult pneumococcal vaccination schedule under the National Immunisation Program (NIP).
From 1 July 2026, the key changes will include:
- The 21-valent pneumococcal conjugate vaccine (21vPCV), Capvaxive, will be added to the NIP
- For adults, 21vPCV (Capvaxive) will replace 13vPCV (Prevenar 13) and the 23-valent pneumococcal polysaccharide vaccine (Pneumovax 23) on the NIP
- A free 21vPCV dose under the NIP will be available for:
- Adults aged 65 years and over
- Aboriginal and Torres Strait Islander adults aged 25 years and over
- Adults aged 18 years and over with specified medical conditions that increase their risk of severe disease
These changes will simplify the schedule, broaden strain coverage and improve protection for more people.
Further information and resources will be published on the Department’s website in the week before the change takes effect.
Access the program advice for health professionals here.
Until 1 July 2026, immunisation providers should continue to recommend and administer adult pneumococcal vaccines in line with the Australian Immunisation Handbook.
Adult pneumococcal vaccination: broadening protection
Presented by National Centre for Immunisation Research and Surveillance (NCIRS)
24 June (10am to 11.30am AWST)
Join this NCIRS webinar for a practical update on pneumococcal disease in adults and the upcoming program changes for immunisation providers. The session will cover:
- The impact of pneumococcal disease in adults
- Current evidence on vaccine safety and effectiveness
- Upcoming changes to the adult pneumococcal vaccination schedule and why they matter
- Practical strategies for preparing for and delivering pneumococcal vaccination
The webinar will also provide practical advice on managing vaccine stock, reducing common errors and responding to patient questions.
Online: register now
Can’t attend live? The webinar will be recorded and published on the NCIRS website. Register now to receive the link in your inbox when it becomes available.
Cancer screening updates
Bowel Cancer Awareness Month

Bowel cancer causes the deaths of 103 Australians each week (5,372 each year), yet it is one of the most treatable cancers when found early.
Although the risk increases with age, bowel cancer can affect people of any age.
Each week, 286 Australians are diagnosed with bowel cancer (14,904 each year).
June is Bowel Cancer Awareness Month and an opportunity to encourage patients to take part in the National Bowel Cancer Screening Program (NBCSP). You can support participation by creating a visible display, offering kits to eligible patients and promoting the program.
Campaign resources are available here.
Clinics can order bowel screening kits through PRODA. Find guidance here.
You can also integrate your clinical software with the National Cancer Screening Register (NCSR) for easier access to patients’ screening information.
Find more information here, or contact WAPHA Project Officer Violet for support with integration at Violet.Corrigan@wapha.org.au
Celebrating 20 years of the National Bowel Cancer Screening Program

This year marks 20 years of the National Bowel Cancer Screening Program (NBCSP). Since it began in 2006, more than 12.8 million Australians have taken part in potentially life-saving bowel screening.
Cancer Council WA has played a leading role in promoting the NBCSP through health promotion, advocacy and activities that raise awareness of bowel cancer and encourage participation.
The full article and timeline of the program from Cancer Council WA is available here.
More information about the National Bowel Cancer Screening Program is available here.
Learn more about bowel screening and Cancer Council WA’s work here.
Education and events
Webinar: Managing chronic kidney disease (CKD) in primary care
Presented by WA Primary Health Alliance
25 June (6.30pm to 7.30pm)
GPs and other primary health care clinicians are invited to join us for the second webinar in this series with Kidney Health Australia.
This webinar will take a deep dive into managing chronic kidney disease (CKD) with a focus on chapter two of the CKD Management in Primary Care handbook (5th edition).
To find out more, view the flyer and register today.
Rockingham Preventative Health Forum – Strengthening immunisation and cancer screening in general practice
Presented by WA Primary Health Alliance
30 June (6pm to 7pm)

WA Primary Health Alliance invites all clinical staff to attend our Rockingham Preventative Health Forum.
This face-to-face event will provide information about the National Immunisation Program (NIP), vaccine safety and administration, and the national cancer screening programs.
To find out more, view the flyer and register for the Rockingham Forum today.
Other Webinars, Events & Workshops
| BreastScreen WA mobile visit to Butler Presented by BreastScreen WA 10 June to 23 December |
| BreastScreen WA mobile visit to Kojonup Presented by BreastScreen WA 10 June to 22 June |
| BreastScreen WA mobile visit to Karratha Presented by BreastScreen WA 11 June to 6 July |
| BreastScreen WA mobile visit to Rangeway (Geraldton) Presented by BreastScreen WA 16 June to 18 June |
| BreastScreen WA mobile visit to Geraldton Presented by BreastScreen WA 19 June to 12 January |
| Talking About Suicide Prevention in Practice – Webinar Presented by Black Dog Institute 20 June |
| Domestic Violence-alert 2-Day Foundations Workshop Presented by Lifeline WA 22 June and 23 June |
| BreastScreen WA mobile visit to Cranbrook Presented by BreastScreen WA 23 June to 25 June |
| Pornography and impact on women’s health webinar Presented by Women’s and Newborn Health Service 24 June |
| BreastScreen WA mobile visit to Tambellup Presented by BreastScreen WA 26 June to 29 June |
| Designated registered nurse prescribing: Pathway to practice Presented by Nursing Midwifery Board of Australia 29 June |
| Endometriosis in Primary Care: Diagnosis, Management and Referral Pathways Presented by RACGP and Goldfields Health Professionals Network 30 June |
| BreastScreen WA mobile visit to Gnowangerup Presented by BreastScreen WA 30 June to 3 July |
| Viral Hepatitis in Primary Care Day – Scholarships available Presented by ASHM 4 July |
| BreastScreen WA mobile visit to Booragoon Presented by BreastScreen WA 6 July to 7 August |
| BreastScreen WA mobile visit to Jurien Bay Presented by BreastScreen WA 9 July to 3 August |
| Ask Us Anything Series – Hepatitis B Edition Presented by ASHM 14 July |
| FDV safety planner webinar Presented by Women’s and Newborn Health Service 12 August |
| Aboriginal Health Conference 2026 Presented by Rural Health West 16 August |
Acknowledgement
WA Primary Health Alliance acknowledges and pays respect to the Traditional Owners and Elders of this country and recognises the significant importance of their cultural heritage, values and beliefs and how these contribute to the positive health and wellbeing of the whole community.
